
We have never needed high-quality data and analytics as much as we do now to underpin the bold decisions required for effective remodelling and integration of health and care. Often we have many different and competing versions of the truth and its hard to determine a single version of the truth on which to make informed partnership decisions.
As all 42 integrated health and care systems (ICSs) formally appoint their chairs, chief officers, boards and executive teams in the coming weeks. There will be enormous pressure on them to evidence their impact to NHSE/I, to politicians and most importantly to local people.
Each ICS has been working across the boundaries of local government, social care, primary care, acute care, physical and mental health in partnership with the community and voluntary sector to wrap support around people and communities. Never has this proved so vital as during the covid pandemic.
There is so much to resolve if we are serious about genuinely integrating our systems, our workforce, our cultures, values, the way we work with communities. So where do we start and how do we prioritise the relative importance of competing priorities?
As the saying goes “If you have 100 priorities – you have no priorities”. Determining a limited number of fundamental deeply transformative change programmes, starting with a clear evidence base for action, is essential.
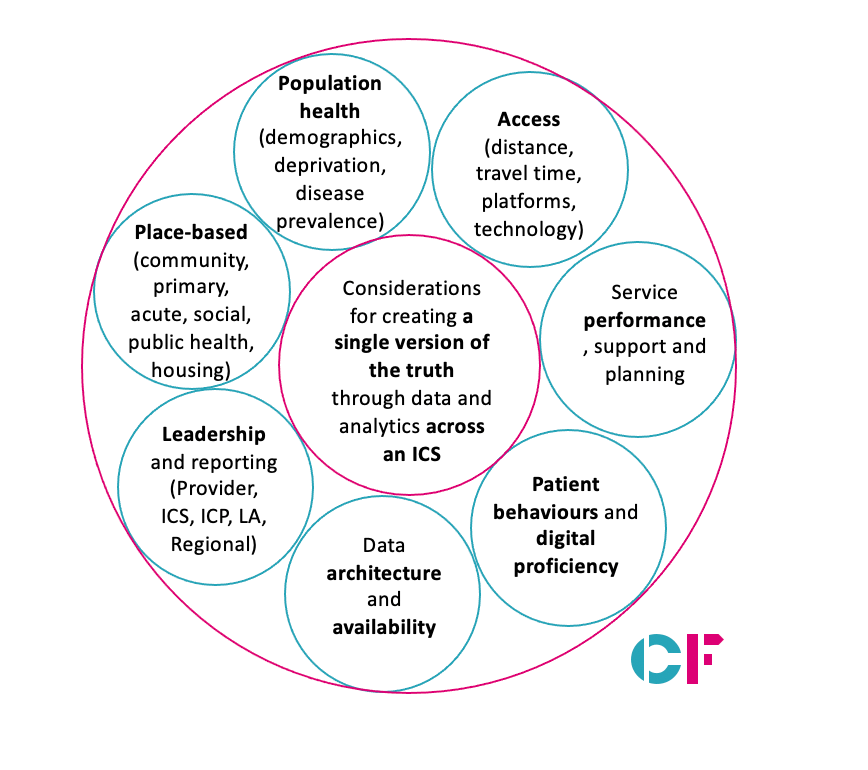
High-quality data and analytics required to build a robust evidence base for action can be in many different parts of the system. It may be within a CCG, a PCN, an ICP, a council’s public health data set, in housing or mental health; importantly it needs to be brought together to prove the clearest of pictures; to tell the deep story of a place. A single version of the truth.
An example of the use of data recently in the Bolton system is the geographical analysis of stillbirths and low birth weight babies across the Borough. There was a concentration of poor maternity outcomes in a few super output areas where maternity services had traditionally been provided in a top-down model from the acute trust. In the Bolton system, we began thinking collaboratively bringing together services with local communities and families. An amazing community outreach midwife, health visitors and GPs set up a local maternity hub providing confidential early advice during pregnancy. We are already starting to see the benefits in the wider system and for local families in the area.
Similarly, in HSJ Partnership of the year, West Yorkshire and Harrogate ICS’ application of innovative data sharing of poor health outcomes and lower life expectancy by up to 20 years for people with learning disabilities led their provider collaborative to tackle their waiting lists together, prioritising people with learning disabilities.
Directors of Public Health produce an annual Joint Strategic Needs Assessment of their local areas underpinned by system data. This is a key document for ICSs to analyse and should be the basis of collective action by all partners with an equal focus on prevention as well as treatment.
It is important that data collection and analysis doesn’t just become an end in itself and that we don’t spend too much time agreeing we have serious problems in poorer communities but that it actually leads to joint collective transformative work in those specific areas with the support and buy-in of the local community and the wider system.
There are bound to be disagreements between partners about the right things to focus on in an ICS but having a single version of the truth as a clear and jointly owned evidence base means there is a framework of reference to draw on when making those tough choices about the allocation of resources, capacity and time.
Whether your role is in a primary care network, an integrated neighbourhood team, a council, an acute trust, the board of an ICS or ICP, a provider collaborative, in housing, the community and voluntary sector or in public health, data is a vital component on the journey to better health and care in local communities.
Chris Ham is chair of the Coventry and Warwickshire ICS and Donna Hall is chair of Bolton NHS Foundation Trust and former CEO of Wigan Council. Chris and Donna are both advisers to CF and members of the board of New Local.


")
