
Released in May 2026, NHS England’s Best Practice Guide for NHS Frailty Pathways sets out what a high-performing system should deliver for people living with frailty. The ambition is a genuine shift: from reactive, hospital-centred care toward earlier identification, better coordination, and community-based support.
What the guidance covers
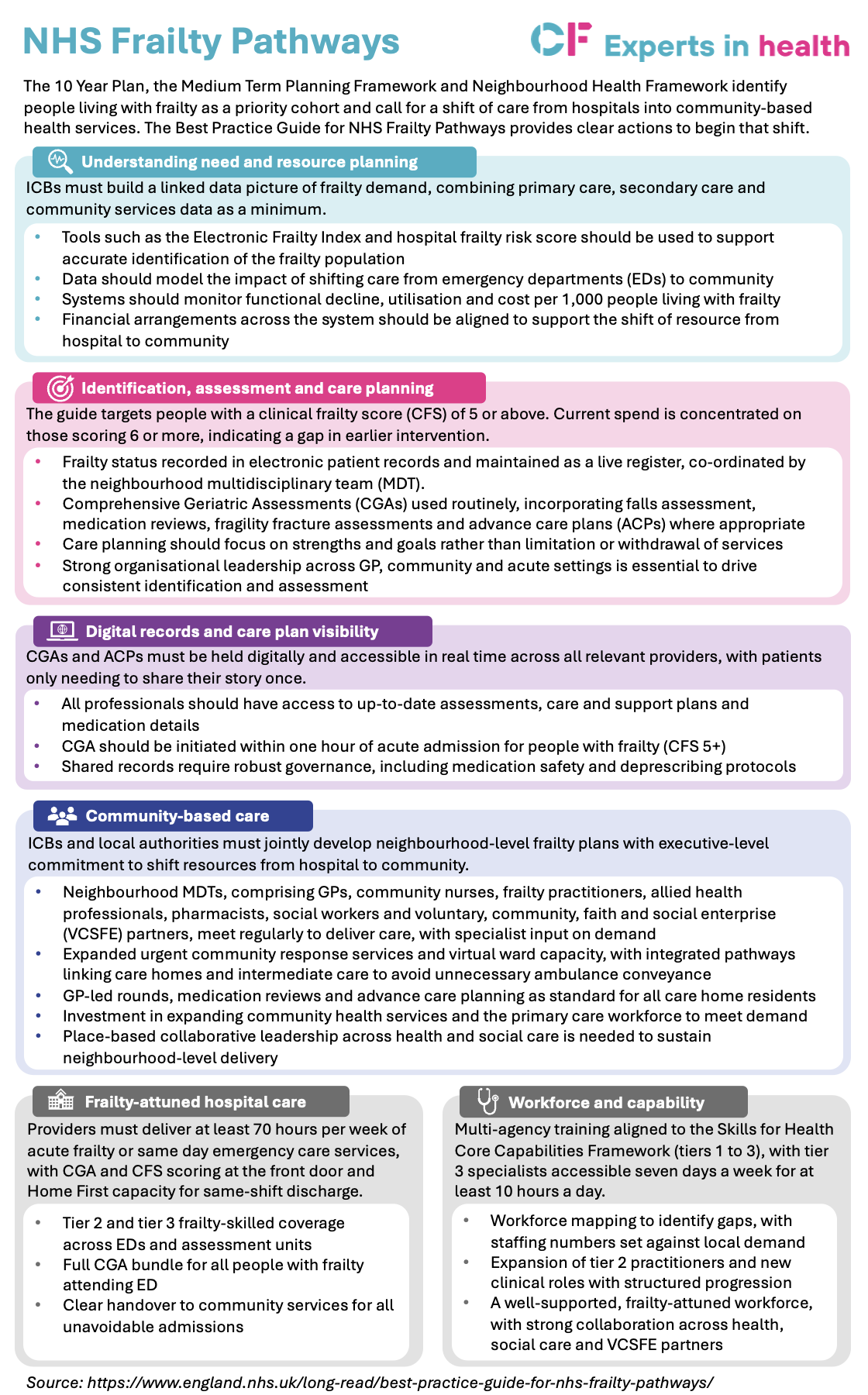
The framework focuses on specific actions: understanding need and resource planning; identification, assessment and care planning; digital records and care plan visibility; community-based care; frailty-attuned hospital care; and workforce and capability. These are underpinned by key enablers below that drive improvements in care for people living with frailty. Across all actions, the direction of travel is consistent. Data should drive decisions. Assessments should be routine, not exceptional. Community infrastructure needs real investment, not just intention. And financial flows need to follow the care model rather than defaulting to acute spend.
The full snapshot below breaks down what the guidance asks of systems across each domain.
Click to expand
FAQ’S: Behind the guidance
The guidance does not ask systems to do something untested – the building blocks exist. What has been missing in many places is the data infrastructure to plan with confidence, the community capacity to manage demand, and the financial architecture to make the shift permanent. Getting those three things right is what separates systems that are making genuine progress on frailty from those that are managing it expensively and reactively.
Read the full guide here.












")
