
Ten years on from the journey to integration
Ten years ago, CF and the Local Government Association published The Journey to Integration: Learning from Seven Leading Localities. The report examined seven English areas that had pursued joined-up care for a decade or more. The results were striking; Northumberland reduced emergency admissions for frail elderly patients by 36%, Torbay halved the rate of growth in health and care costs against the national trend and Tower Hamlets increased the share of diabetes patients with a care plan from 10% to 88%. Thanks to integrated care, these gains were not marginal.
A decade on, the 10 Year Health Plan reaffirms the same ambition: shift care from hospitals to communities, from sickness to prevention, build neighbourhood services around populations rather than buildings. And this time leverage the full potential of the technology revolution, shifting analogue to digital.
But there is a lost decade in between when the report was published in 2016 and today in 2026 which has stalled or unravelled some of the progress that was being made in the decade preceding the report (from 2006 to 2016). Overall, as Darzi noted the aspiration for a “left shift” to prevention saw the opposite or a “right drift” with a 10 percentage point increase in hospital spending at the expense of primary and community care. Local Authority funding fell up to 40% making the funding of social care more difficult. Organisations changed: Torbay Care Trust, for example, no longer exists as it was done away with as a result of reforms. Payment reform did not just stall but reversed block budgets put in place of “payment by results” which eliminated the inherent incentive in avoiding hospital care. Commissioning was denuded.
The government once more seeks to anchor around the theme of preventative health, this time labelled Neighbourhood Health.
The original report remains relevant
The seven case studies identified key questions that need to be addressed to make that integration ambition deliverable:
- Impact: what is the level of ambition?
- Place: how challenging is the context in health needs?
- Focus: what cohorts and what services are in scope?
- Care model: what changes need to be made to the model of care?
- Information: how does information flow support care, patient engagement, performance or payment?
- Commissioning: what changes in spending and payment models are needed?
- Workforce: what changes in workforce numbers, roles, skills and ways of working are required?
- Governance: what changes are needed to organisational function and form?
- Leadership: how long is the history of joint working and how deep is the engagement and commitment?
Five observations from a decade’s hindsight are worth remembering as the health system reverts to a focus on healthcare value.
1. The impact was real, and it was repeatable
The original case studies were not outliers. In North West London, and North East London, each covering a population of around 1.5 to 2 million, sustained a 40% reduction in emergency admissions in the inner boroughs that adopted integrated care, against a 10% increase in outer boroughs that did not (CF analysis). The original finding, that meaningful integration takes 10 to 15 years to embed but produces double-digit impact when it does, has held up in the data in the UK as well as in multiple examples from around the world of similar levels of achievement.
Examples of a PHM approach have been pursued in Inner North East and Inner North West London, showing 40% decrease vs 10-20% increase elsewhere

Note: 2020/21 smoothed for indexed cost. Source: UK House of Commons Research Briefing: NHS funding and expenditure (2024), Populations data is from ONS. Spend by care setting is taken from Darzi report (2024), 2021/22 – 2023/24 splits are assumed to 2020/21 proportions documented in Darzi. Between 7-10% of spend categorised as ‘Other’ and not attributed to any care setting.
2. Focus on the drives of healthcare utilisation, not the whole population
The original report noted that what England calls ‘integrated care’ is more commonly known elsewhere as ‘Population Health Management’. More recently, the UK government has adopted the term ‘Neighbourhood health’. Whatever the label, successful models do not target the whole population equally. Instead, they focus on the groups that drive the greatest healthcare use and experience the largest outcome gaps. These groups typically include people with chronic conditions, whether single long-term conditions or multimorbidity, and frail older people. In most cases, 10–20% of the population accounts for 50–80% of costs.
A common mistake is choosing either too narrow a cohort to achieve meaningful impact or too broad a focus to be practical. The first usually comes from designing a model that feels easier to deliver; the second from conflating population health management with population health or public health more broadly.
Evidence from across England now shows the same pattern at population level: the 80/20 rule is clearly visible. For example, people with chronic conditions and dementia represent 21% of population and drive 64% of costs, and 24% of the population drive 86% of hospital costs.
Distribution across segments by population, total cost, and activity (all ages) 2024

Source: CF Health Strata, HES, Provider NCC 24/25 – MFF Adjusted
3. Design the care model around the needs of groups in focus
Beyond providing a pragmatic focus on addressable cost, focus is critical for designing the appropriate model of care. While common themes exist about need to identify and close care gaps, focus on individual, coordinate care, etc the precise interventions, intensity of support, need for diagnostics and therapeutics, scale of delivery, vary significantly:
- Single long-term conditions need case finding and diagnosis and put on appropriate treatment and ensure adherence.
- Multimorbidity shares these needs but has need to understand comorbidity and polypharmacy.
- Frail/elderly have need to engage with carers and families, consider falls prevention, and ways of keeping people socially active.
- Severe mental illness needs a focus on housing and employment, integration with policy and A&E and establishment of community-based crisis intervention.
The case examples in the original report showed this:
- Tower Hamlets began with 11,000 diabetic patients, 4% of the population, then extended its reach to 20% by including all chronic conditions. The programme started in primary care and has since expanded into public health, community health, and mental health.
- Torbay concentrated on older people in the top 10% at risk, alongside chronic disease, with community health and social care as the primary delivery vehicles. Primary and acute providers were brought in subsequently.
- Pennine Care’s RAID model targeted people with mental health needs, working across secondary and community care settings.
- Salford, Leeds, and Nottingham City each address a broader spectrum, covering older people and those with chronic conditions, with a consistent focus on primary, community, and social care integration.
- Northumberland has focused on frail elderly people at high risk of admission, around 3% of the population, delivered through primary care and community locality integrated networks.
The original report mapped out the range of different interventions needed:

Source: Richardson, Journey to Integration (Local Government Association and CF, 2016)
Today, we would sharpen this observation and say that the critical common element across different segments is the need to apply a data-driven targeted approach to identify and close care gaps.

Source: CF PHM analysis
And we have shown in recent research that 10 years on, these gaps have not closed.
Diagnosis and treatment gap in CVD, diabetes, obesity, CKD and dementia
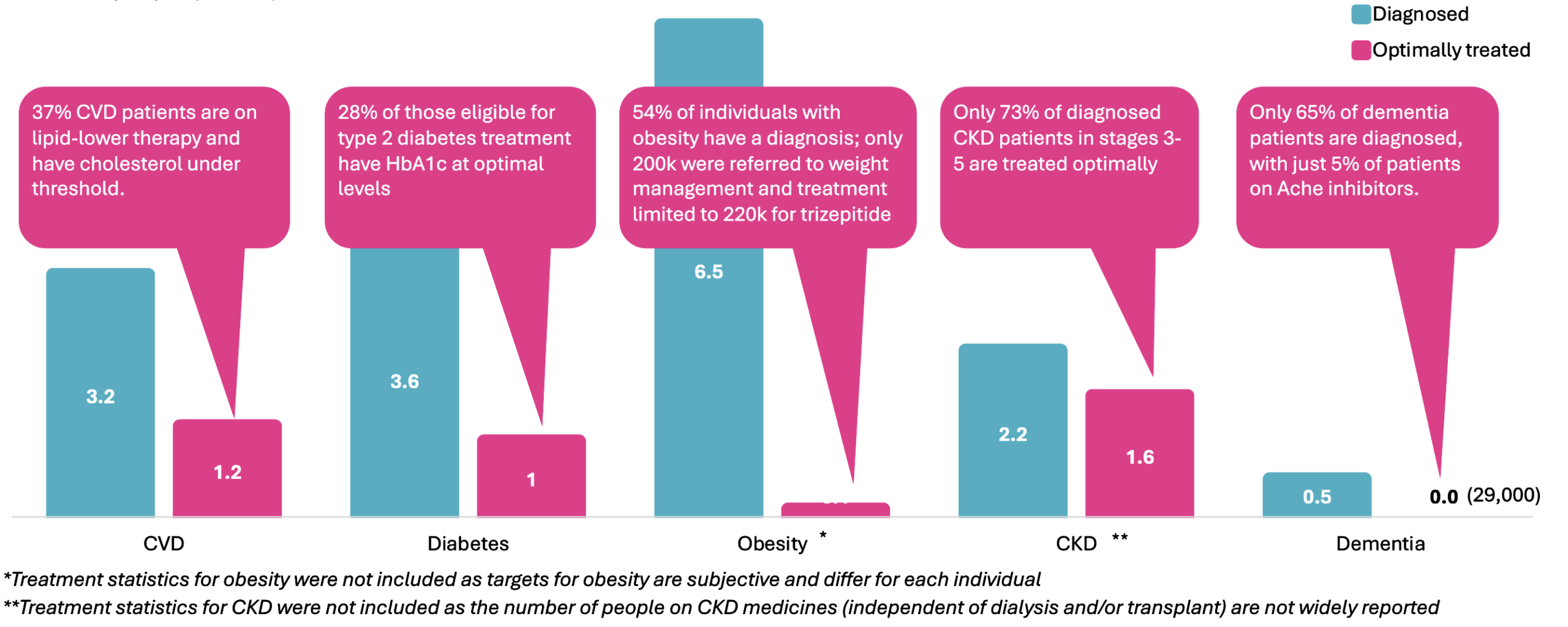
Sources: Richardson, Oviosu, Andrews, Unmet Care Gaps (CVD: CVDPREVENT, Health Survey England; NHSBSA; British Heart Foundation; Diabetes: QOF, NHSE, ONS; Obesity: Gov.UK, QOF, National Obesity Audit; CKD: Kidney Research UK, QOF; Dementia: NHSE Primary Care Dementia Data, DiscoverNOW, QOF, CF analysis)
4. Access to integrated data is critical
Jack Cochrane, the President of Kaiser Permanente Medical Group, inspired change in the UK by telling clinicians and managers “it is impossible to have integrated care if you don’t know someone’s phone number.”
Mature integrated care programmes share several informatics characteristics: robust information governance, shared care records, near real-time patient data, and information systems that underpin payment mechanisms and performance tracking. Clinicians, staff, and patients all have access to shared records and diagnostic results through appropriate controls, with patients able to input their own data for goal-setting and monitoring. Telemonitoring, telemedicine, and emerging technologies support new care models and joined-up working.
Tower Hamlets was fortunate to have far sighted clinicians who established a clinical effectiveness group that integrated primary care and acute care information for supporting clinical audit; they had what was needed and agreed that population health management was a suitable purpose to extend to, enabling case finding and care coordination as well as performance tracking and incentives.
North West London had not originally had the information sharing in place, but in order to be able to perform what was required of its “Whole System Integrated Care” it undertook to create this. The information governance to enable this was put in place with an arrangement for patient identifiable data for clinicians in contact with patients and a pseudonymised copy for use for population health management, system management and research. Every provider – including nine NHS trusts and more than 400 GP practices as well as eight boroughs, all signed a Data Sharing Agreement endorsing these arrangements. A shared controller model was established which enabled a committee to approve specific uses without recourse to amending the agreement for every new use.
The original report noted, however, implementation falls well short of this ambition. Many programmes have adopted one or more informatics tools; shared care records, patient-level datasets, or telemonitoring, but few have achieved genuine interoperability across care settings. Fewer still have deployed telemonitoring or telemedicine at scale, and very few have yet used data to drive payment or performance management.
It is often said that there is an Information Governance problem enabling the integration of primary care with hospital and other data. That’s not really true. GDPR gives the system everything it needs, albeit requires the engagement of patients and public and agreement of the data controllers, making the agreement of General Practice critical. North East London, North West London and Greater Manchester have solved the problem at scale across populations of millions. They did so through engagement of GPs to sign data sharing agreements with every provider, allowing the sharing of data for patient care, risk stratification, system management and research. The real motivation in London was to be able to achieve integrated care. The motivation to achieve this was enhanced with addition funding and incentives for primary care.
The unfinished task is putting the model in place elsewhere. For many years, people have looked for a shortcut around this. There is no shortcut. What causes GPs to share data is alignment with the purpose of population health management (PHM) and the incentives that follow. Where that alignment exists, the data flows. Where it does not, no technical or contractual fix substitutes for it.
5. Changes in the flow of money are critical
A contract that pays for a whole population but cannot track what happens to individuals within its practice is just a lump-sum payment with no accountability attached. That remains the simplest practical test of whether a population-based contract is operating as intended.
Transformation cannot happen without adequate resources. Primary care sits at the centre of most care models, and the additional funding it requires must be recognised and provided. Payment reform should follow a clear vision for change, not precede it. Where it has succeeded, new models have been developed collaboratively and implemented over several years.
Three specific shifts require payment reform to enable them: funding upfront activity for prevention and proactive care, such as care planning and coordination; facilitating patient flow across primary, acute, community and social care settings; and incentivising clinicians and providers to work in ways that deliver system-wide value.
Examples included:
- Tower Hamlets prioritized five chronic conditions plus vaccines, developed care packages, spelling out the interventions needed with frequency, time, and level of workforce, and then determined the number of people in each primary care network in each condition and the level of funding that would be needed to deliver this model. It paid 70% of that money up front and 30% based on performance. Performance included the capture of data, the number of care plans developed, and improvement in outcomes.
- In inner North west London, a similar approach was taken as Tower Hamlets, with the definition of segments of population, an initial focus on elderly and diabetes, and the development of these care packages. It focused on additional resources for care coordination, multidisciplinary team meetings, and the engagement of specialists from the acute hospital. The payment model here incentivized this activity directly, for instance paying £37.50 for each care plan developed based on an assumption of 45 minutes of clinician time, and paying for hospital consultants to have a hotline to answer and provide specialist opinion while a GP was with a patient. It also created a pot of money from the avoidance of emergency admissions, which was shared between the hospital and GP practices upon achievement of results.
- Torbay operated as a care trust with a pooled health and social care budget, which proved a significant enabler of integration. The 2012 reforms dismantled this model, separating payment from provision and splitting social care from healthcare budgets. The subsequent creation of an integrated care organisation has since overcome that barrier.
- Northumberland’s Locality Integrated Networks were built on risk-sharing arrangements between the CCG, local authorities, and providers. The Frail Elderly Pathway drew on a range of funding streams to support its operation.
The 2016 case studies all required new investment up front: community workforce, diagnostics, medicines, technology, and programme costs. The savings that justify that investment must be released from acute care. It remains a wicked problem to spend more on these investments and to recover the savings in acute care next year.
When Payment by Results was paused in 2020, it halted savings from non-elective admissions flowing back to fund resources outside of hospital needed to produce the savings. Activity-based payment has now restarted, and the link is reconnected. Going forward, any reduction in hospital demand will translate into lower spending on hospitals.
The 2016 conclusion remains valid once again: No legal or policy barriers prevent new payment models from being introduced. The 10-year plan pointed to “year of care budgets” and multiyear settlements but these do not exist yet.The obstacles are practical: gaps in coordination, leadership, and technical knowledge. The skills needed to design and operate new payment models are substantial and currently scarce.
Taken together, this points to one conclusion: significantly more resource, leadership attention, and technical capability need to be directed at payment reform.
6. The localities that succeeded built in the right order
The localities that delivered the largest impact followed a sequence: shared vision and a leadership coalition first; care model redesign second; data and information governance third; contractual and organisational change last. Form follows function. Tower Hamlets’ GP networks became formal organisations only when the volume of money and risk channelled through them required it. Northumbria’s vertical integration of community and acute care followed years of joint working.
The Integrated Health Organisation agenda provides the opportunity to set more areas on the path to integration. The areas that land it well will be those that build the leadership coalition, data foundation and care model investment before, rather than after, the contractual and governance changes.
Applying the lessons from the past to today’s priorities
The lesson from the 2016 case studies is that the neighbourhood team model works when it is configured to deliver specific, measurable changes in activity. Tower Hamlets’ GP networks delivered care packages for diabetes that reduced acute exacerbations. North West London delivered improvements not just in diabetes and elderly care but across the key drivers of demand. Northumberland’s frail elderly pathway reduced a defined cohort of emergency admissions.
The current generation of neighbourhood teams will deliver most when they are pointed at the same kind of specific, financially relevant operational targets. The NHS today operates against a tighter and more specific set of priorities than it did in 2016. Reducing urgent and emergency care demand and outpatient demand is now central to delivering the constitutional standards on A&E performance and the 18-week elective pathway. Integrated neighbourhood teams can provide the operational vehicle through which the 10 Year Health Plan expects this to happen. They need to understand what level of impact they can have, in what cohorts of people and hence
Three developments since 2016 sharpen the original PHM logic the case studies were built around. Digital and AI tools allow patients to be engaged, health encounters to be delivered, disease to be predicted and results to be tracked without consultations. The 2016 case studies achieved their outcomes within the constraints of the consultation model. The next phase will not.
The focus on guideline-directed protocols has tightened. Precise inclusion and exclusion criteria, applied to integrated population data, identify individuals with known care gaps or significant clinical risks automatically rather than opportunistically.
The framing has tightened too. The original integrated care agenda placed extensive emphasis on building shared vision across whole geographies, that work remains valuable. The tighter financial envelope means the operational focus needs to be sharper: on the specific cohorts whose care delivers reduced urgent and emergency and outpatient activity, and improved outcomes.
The seven localities profiled in 2016 had each begun the journey at least a decade before publication. The destination they were heading toward is the destination the system is heading toward now. With better data, sharper protocols and clearer financial logic, the system has never been better equipped. The time to act is now.
About CF
CF is a leading consultancy dedicated to making an enduring impact on health and healthcare. We work with leaders and frontline teams to improve health, transform healthcare, embed life science innovation and boost growth through investment. With unmatched access to UK healthcare data and award-winning data science expertise, our team are a driving force for delivering positive and meaningful change.
About the authors
")
Ben Richardson
Ben Richardson is a Managing Partner at CF, leading Life Sciences and Data Innovation. With two decades of experience, he has worked with health systems and life sciences companies to improve population health leveraging data digital and AI. Ben has contributed to primary care, diabetes, cardiovascular, cancer, mental health, and population health management. Since 2014, he has helped CF become an award-winning healthcare company in management consulting and data services.










")
