
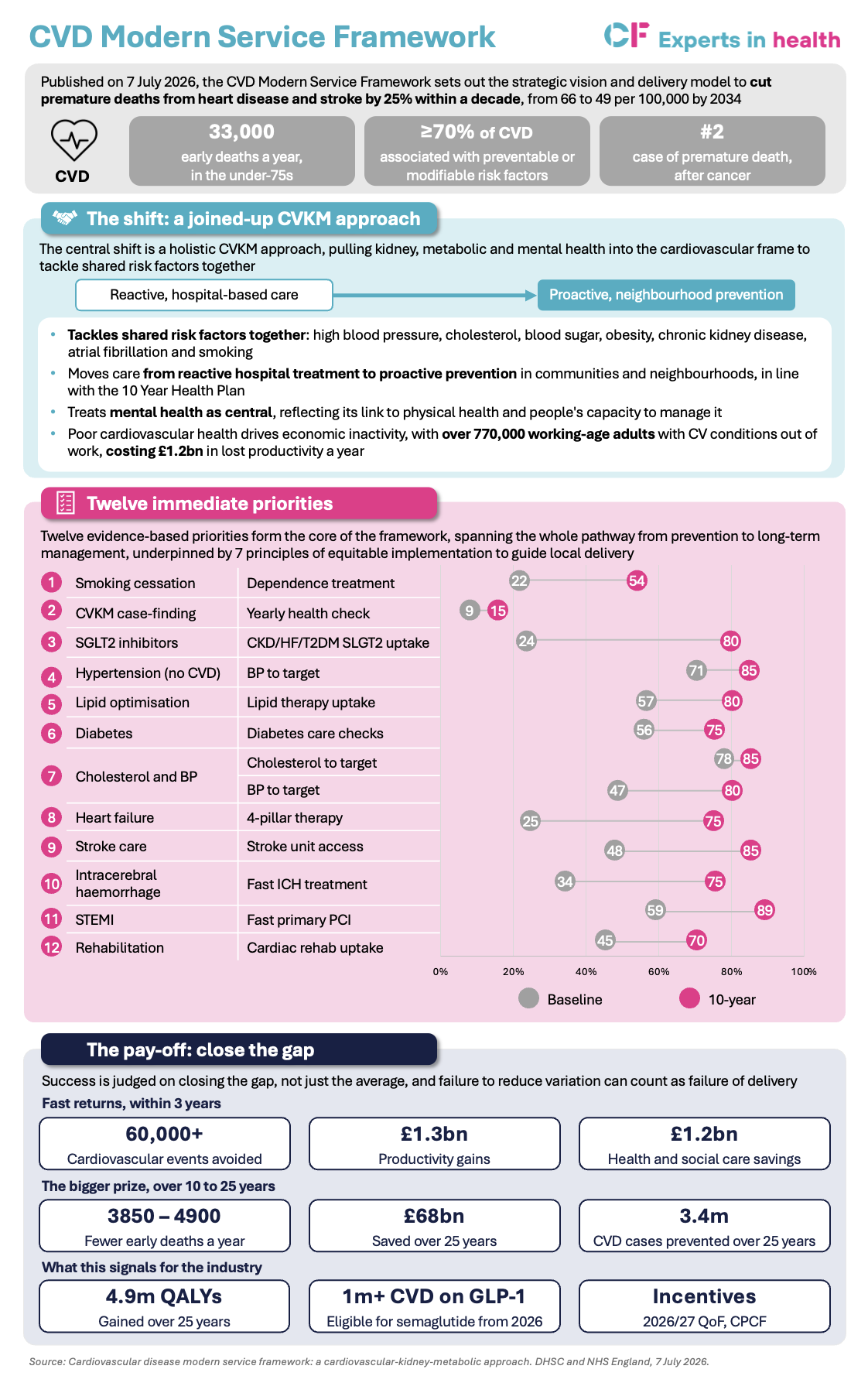
Heart disease and stroke still cause around 33,000 premature deaths a year in England, second only to cancer, and most are preventable. On 7 July 2026, the Department of Health and Social Care and NHS England jointly published the cardiovascular disease modern service framework (CVD MSF), the first of the modern service frameworks committed to in the 10 Year Health Plan. It sets a single, measurable ambition: cut premature deaths under the age of 75 from heart disease and stroke by a quarter within a decade.
What the framework does
The framework does three things: reorganises cardiovascular care around a core principle, highlights 12 priorities where the evidence is strongest and delivery today is most inconsistent, and holds integrated care boards (ICBs) and local government accountable for outcomes.
The core principle is a cardiovascular-kidney-metabolic (CVKM) approach. High blood pressure, high cholesterol, high blood sugar, obesity, chronic kidney disease, atrial fibrillation and smoking share causes, cluster in the same people, and drive most heart attacks and strokes. Managing them together, rather than through separate condition pathways, is where the framework expects the largest reduction in premature mortality.
At least 70% of cardiovascular disease is associated with preventable or modifiable risk factors. And the burden is unequal: people in the most deprived communities are four times more likely to die from cardiovascular disease, and to die earlier. The framework aims to “find the missing millions” who live with undiagnosed or unmanaged risk, and shift that care from reactive, hospital-based care to proactive, neighbourhood-based care.
The 12 priorities focus effort where the evidence for cutting early deaths is strongest and where delivery today varies most. They fall under 4 themes; finding the missing millions, driving treatment to target, timely, equitable acute care and expanding access to cardiovascular rehabilitation.
Several of these start from a long way back, with delivery partners expected to improve year on year. . Each priority carries a baseline, a three-year target and a 10-year ambition, so systems have both a near-term milestone and a longer trajectory to plan against. The three-year target is the marker of early progress; the 10-year ambition is the fuller stretch goal. Closing gaps like these means delivering consistently where performance today is patchy.
The delivery model holds ICBs and local government accountable for outcomes, each ICB names a clinical lead for CVKM delivery, with a national board and regional teams providing oversight. Crucially, every standard carries a variation metric, and the framework states that failing to close the gap between best and worst performers could count as a failure of delivery, whatever the overall numbers. The priorities are already live, aligned to 2026/27 incentive schemes including the Quality and Outcomes Framework and acute Best Practice Tariffs.
See the snapshot for a full breakdown:
Click to expand
FAQ’S: Behind the framework
The framework’s risk is delivery, not strategy. The harder work is operational: turning condition-based registers into a single CVKM view of the population, standing up neighbourhood case-finding that reaches people currently missing from services, and building the data to track variation at practice level.
To read the full CVD modern service framework, click here.
The framework’s risk is delivery, not strategy. The harder work is operational: turning condition-based registers into a single CVKM view of the population, standing up neighbourhood case-finding that reaches people currently missing from services, and building the data to track variation at practice level.
To read the full CVD modern service framework, click here.











")
