
The 2026 Health Bill is one of the most significant pieces of NHS legislation in over a decade. Introduced on 14 May 2026, it sets out a fundamental reshaping of how the NHS is led, governed and held to account. The abolition of NHS England sits at its centre, but the implications run deeper than any single organisational change.
The Bill rewrites who holds commissioning power, who regulates providers, and who owns the data. For NHS leaders, commissioners and those working commercially with the NHS, the architecture has materially changed.
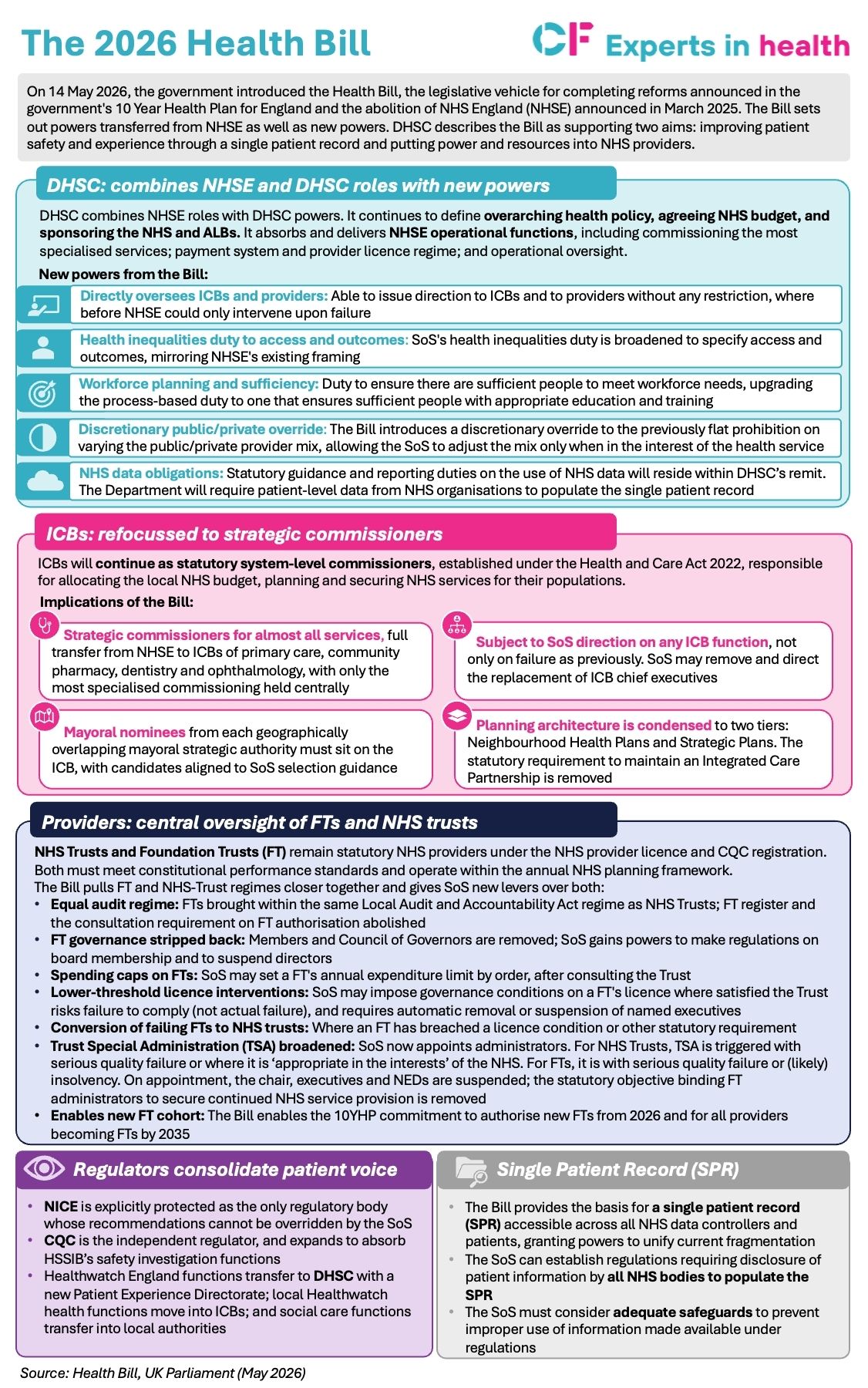
What the Bill does
For NHS leaders, the implications are far-reaching. The new bill makes DHSC the operational headquarters of the NHS, absorbing commissioning of primary care, specialised services, secondary dental, public health and screening from NHSE. The department will now directly administer functions it previously delegated. The Secretary of State holds new powers to issue direction on ICB commissioning decisions, cap Trust spending, and vary or revoke Foundation Trust licences.
It also repositions ICBs as strategic commissioners of almost everything, including primary care, community pharmacy, dentistry and ophthalmology, with boundaries realigning to strategic authorities. The Integrated Care Partnership is abolished. System architecture simplifies to neighbourhood and strategic tiers.
For the commercial market, the implications are significant. The single point of accountability for commissioning decisions shifts from NHSE to DHSC. The access pathway for life sciences, the investment thesis for health infrastructure, and the procurement landscape for health technology all need to be re-read against the new architecture.
The single patient record adds another layer. A unified data spine across GP, hospital and community records, accessible to patients through the NHS App, creates a new substrate for digital health products and services.
A snapshot of the 2026 Health Bill: CF’s latest snapshot focuses on the provisions most relevant to NHS leaders and executives: what is changing, when, and what it may mean in practice.
Click to expand
FAQ’s: Behind the guidance
The structural logic of the Bill is clearer than at any point in the past two decades. Translating that into operational reality will take longer. Commissioning capability, financial stability and organisational confidence do not transfer automatically. Understanding where decisions will actually sit, and who will make them is the more useful starting point.
To see the 2026 Health Bill in full, click here.
The guidance does not ask systems to do something untested – the building blocks exist. What has been missing in many places is the data infrastructure to plan with confidence, the community capacity to manage demand, and the financial architecture to make the shift permanent. Getting those three things right is what separates systems that are making genuine progress on frailty from those that are managing it expensively and reactively.
Read the full guide here.












")
